
Cardiovascular system examination OSCE Guide
CARDIOVASCULAR EXAMINATION – OSCE GUIDE

Cardiovascular examination frequently appears in OSCEs. You’ll be expected to pick up the relevant clinical signs using your examination skills. This cardiovascular examination OSCE guide provides a clear step by step approach to examining the cardiovascular system, with an included video demonstration.
Introduction
Wash hands
Introduce yourself
Confirm patient details – name / DOB
Explain the examination
Gain consent
Position the patient at 45° with their chest exposed
Ask if the patient has any pain anywhere before you begin!
General inspection
Bedside – treatments or adjuncts? – GTN spray / O2 / medication / mobility aids
Comfortable at rest? – does the patient look in pain?
Shortness of breath at rest?
Malar flush – plum red discolouration of cheeks – may suggest mitral stenosis
Inspect chest – scars or visible pulsations?
Inspect legs – harvest site scars / peripheral oedema / missing limbs or toes

General inspection
Hands
Hands out with palms facing downwards
Splinter haemorrhages – reddish / brown streaks on the nail bed – bacterial endocarditis
Finger clubbing:
Ask the patient to place the nails of their index fingers back to backIn a healthy individual you should be able to observe a small diamond shaped window (Schamroth’s window)When finger clubbing is present this window is lostFinger clubbing has a number of causes including infective endocarditis and cyanotic congenital heart disease
Hands out with palms facing upwards
Colour – dusky bluish discolouration (cyanosis) suggests hypoxia
Temperature – cool peripheries may suggest poor cardiac output / hypovolaemia
Sweaty/clammy– can be associated with acute coronary syndrome
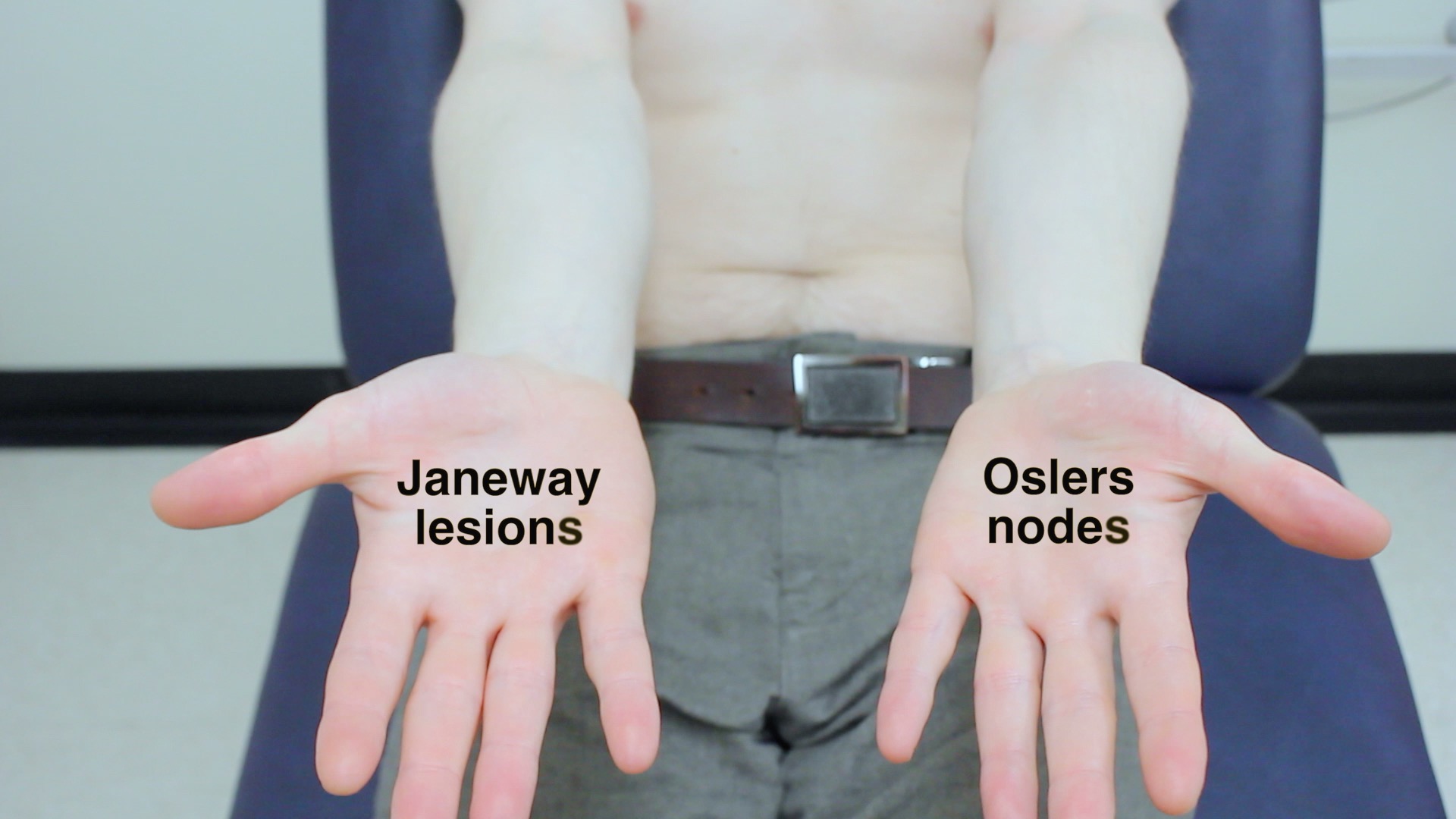
Janeway lesions – non-tender maculopapular erythematous palm pulp lesions – bacterial endocarditis
Osler’s nodes – tender red nodules on finger pulps / thenar eminence – infective endocarditis
Tar staining – smoker – risk factor for cardiovascular disease
Xanthomata – raised yellow lesions – often noted on tendons of wrist – caused by hyperlipidaemia
Capillary refill time – normal is <2 seconds – if prolonged may suggest hypovolaemia

Inspect nails

Assess for finger clubbing

Inspect palms

Assess capillary refill time
Pulses
Radial pulse – assess rate and rhythm
Radio-radial delay:
Palpate both radial pulses simultaneouslyThey should occur at the same time in a healthy adultA delay may suggest aortic coarctation
Collapsing pulse – associated with aortic regurgitation
First ensure the patient has no shoulder painPalpate the radial pulse with your hand wrapped around the wristRaise the arm above the head brisklyFeel for a tapping impulse through the muscle bulk of the arm as blood empties from the arm very quickly in diastole, resulting in the palpable sensationThis is a water hammer pulse and can occur in normal physiological states (fever/pregnancy), or in cardiac lesions (e.g. AR / PDA) or high output states (e.g anaemia / AV fistula / thyrotoxicosis)
Brachial pulse – assess volume and character
Blood pressure:
Measure blood pressure and note any abnormalities – hypertension / hypotension
Narrow pulse pressure is associated with aortic stenosisWide pulse pressure is associated with aortic regurgitationOften you won’t be expected to actually carry this out (due to time restraints) but make sure to mention that you’d ideally like to measure blood pressure in both arms
Carotid pulse:
Assess character and volume – e.g. slow rising character in aortic stenosisIt’s often advised to auscultate the carotid artery for a bruit before palpating, as theoretically palpation may dislodge a plaque which could lead to a stroke

Palpate radial pulse

Radial-radial delay

Palpate brachial pulse

Collapsing pulse

Measure BP

Palpate carotid pulse
Jugular venous pressure (JVP)
1. Ensure the patient is positioned at 45°
2. Ask patient to turn their head away from you
3. Observe the neck for the JVP – located inline with the sternocleidomastoid
4. Measure the JVP – number of cm from sternal angle to the upper border of pulsation
Raised JVP may indicate – fluid overload / right ventricular failure / tricuspid regurgitation
Hepatojugular reflux:
Apply pressure to the liverObserve the JVP for a riseIn healthy individuals this should last no longer than 1-2 cardiac cycles (it should then fall)If the rise in JVP is sustained and equal to or greater than 4cm this is a positive resultA positive hepatojugular reflux sign is suggestive of right sided heart failure / tricuspid regurgitation

Observe for a raised JVP

Assess for hepatojugular reflux
Face
Eyes
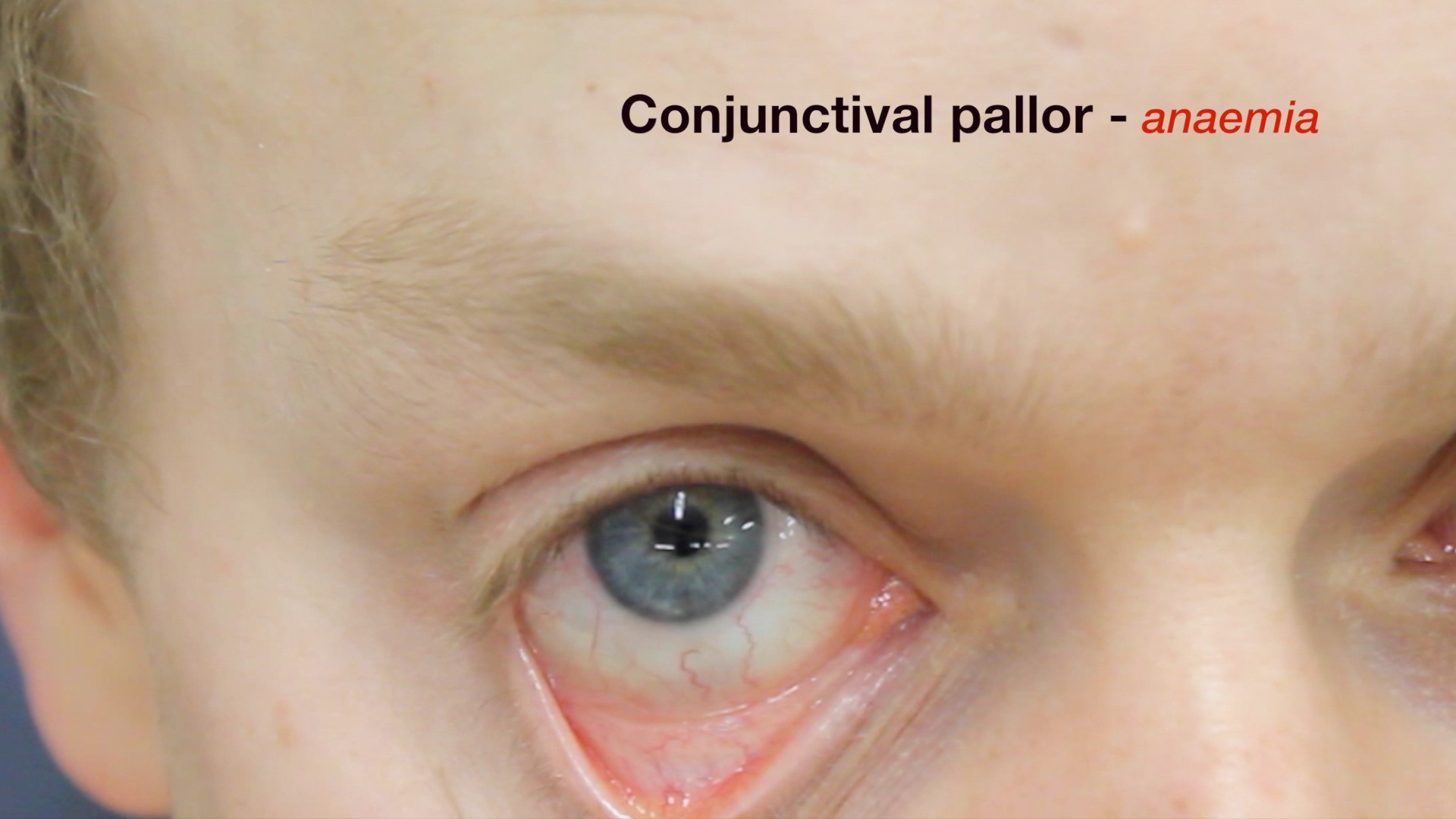
Conjunctival pallor – anaemia – ask patient to gently pull down lower eyelid
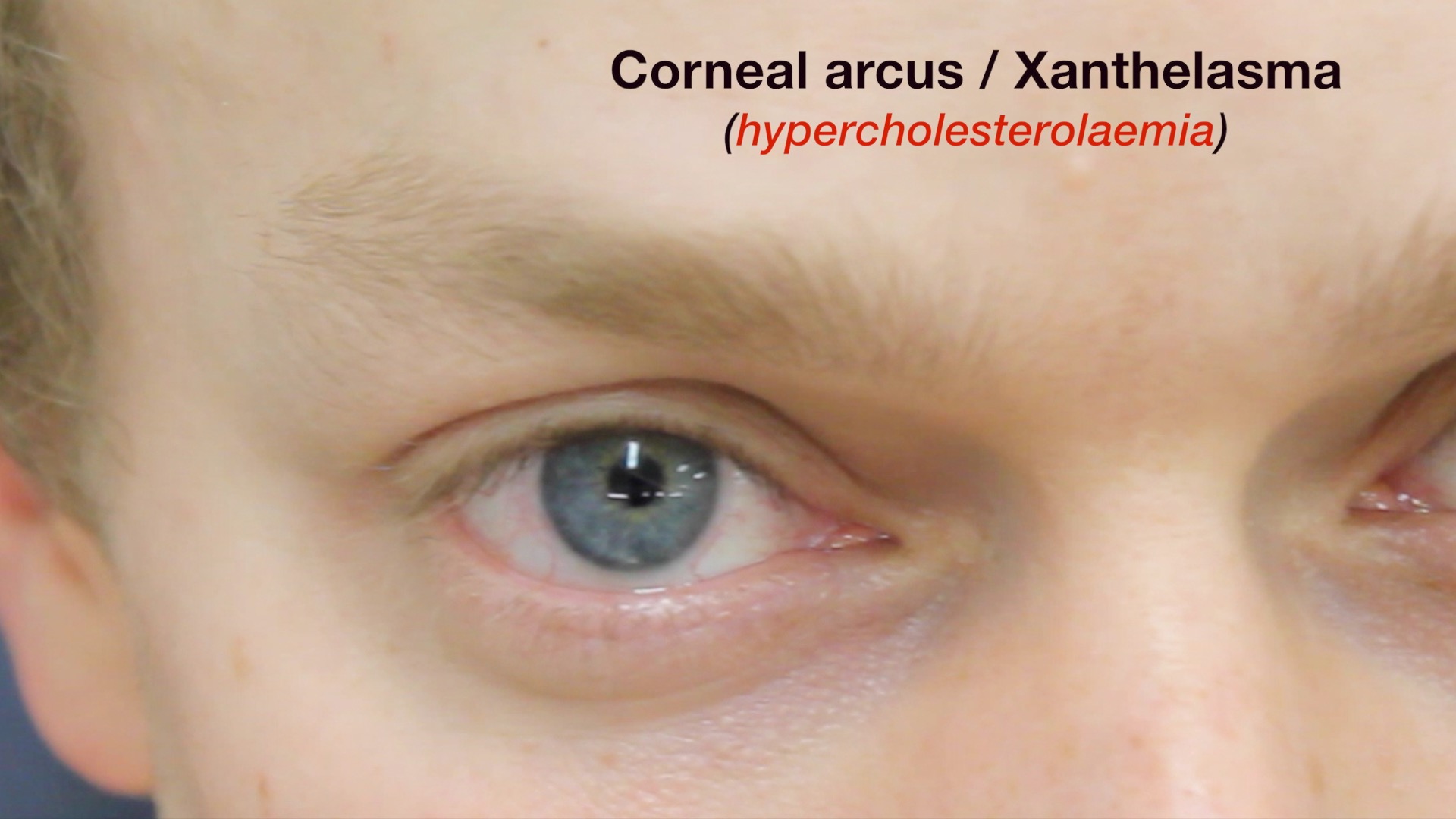
Corneal arcus – yellowish/grey ring surrounding the iris – hypercholesterolaemia
Xanthelasma – yellow raised lesions around the eyes – hypercholesterolaemia
Mouth
Central cyanosis – bluish discolouration of lips / underneath tongue
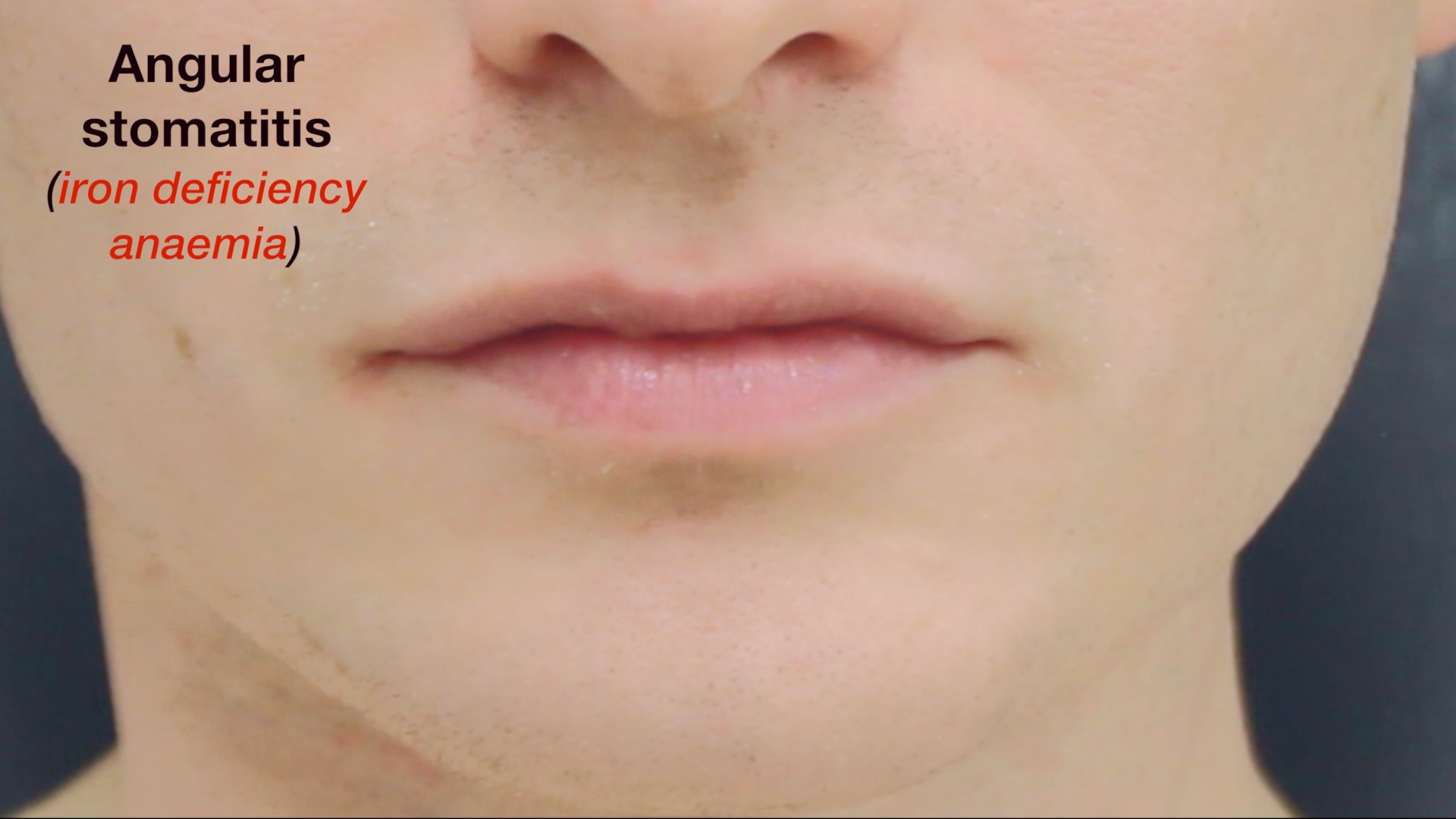
Angular stomatitis – inflammation of the corners of the mouth – iron deficiency
High arched palate – suggestive of Marfan syndrome – ↑ risk of aortic aneurysm/dissection
Dental hygiene – important if considering sources for infective endocarditis

Inspect eyes

Inspect conjunctiva

Inspect mouth

Inspect for central cyanosis
Close inspection of the chest
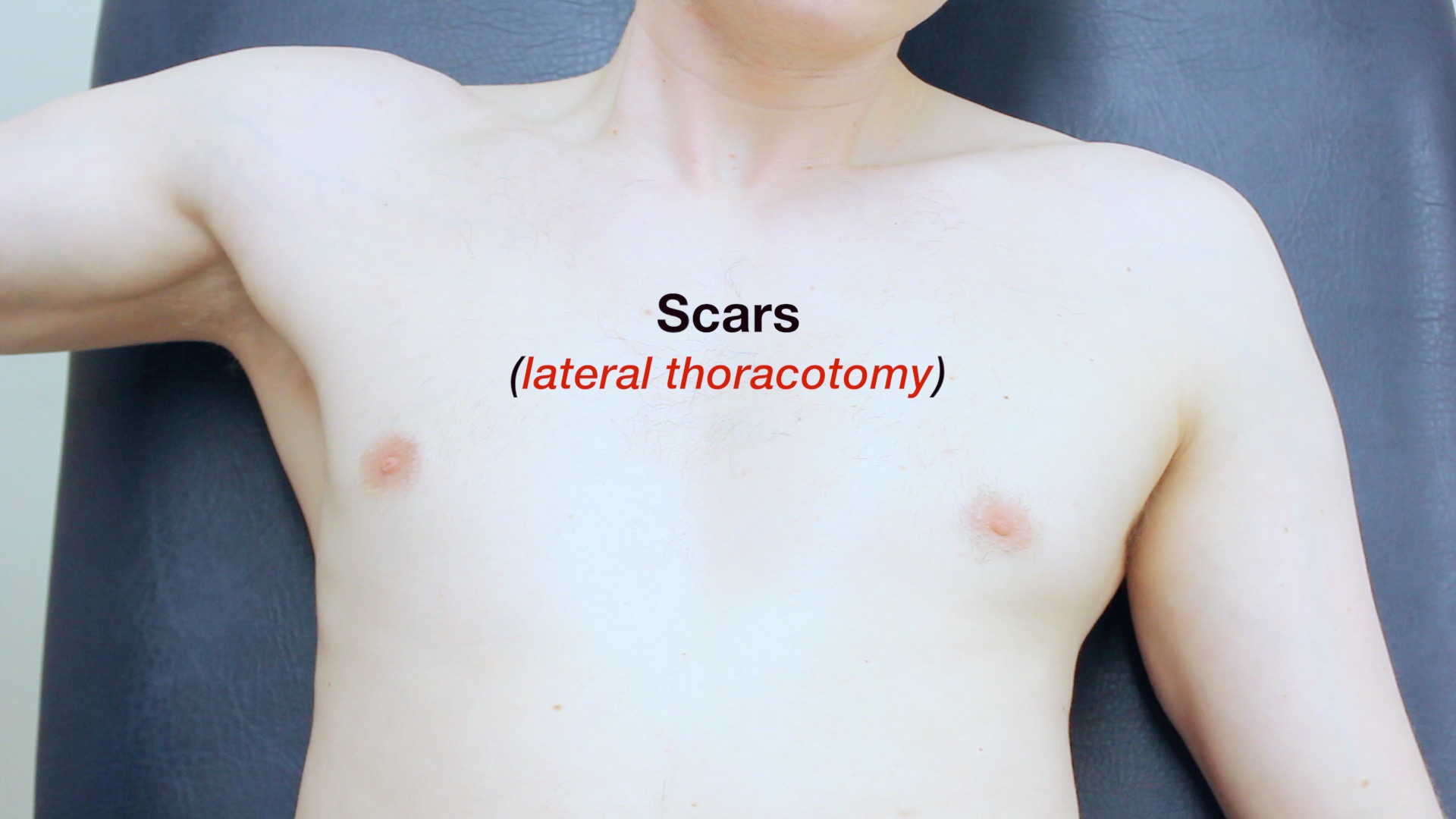
Scars:
Thoracotomy – minimally invasive valve surgerySternotomy – CABG / valve surgery Clavicular – pacemaker
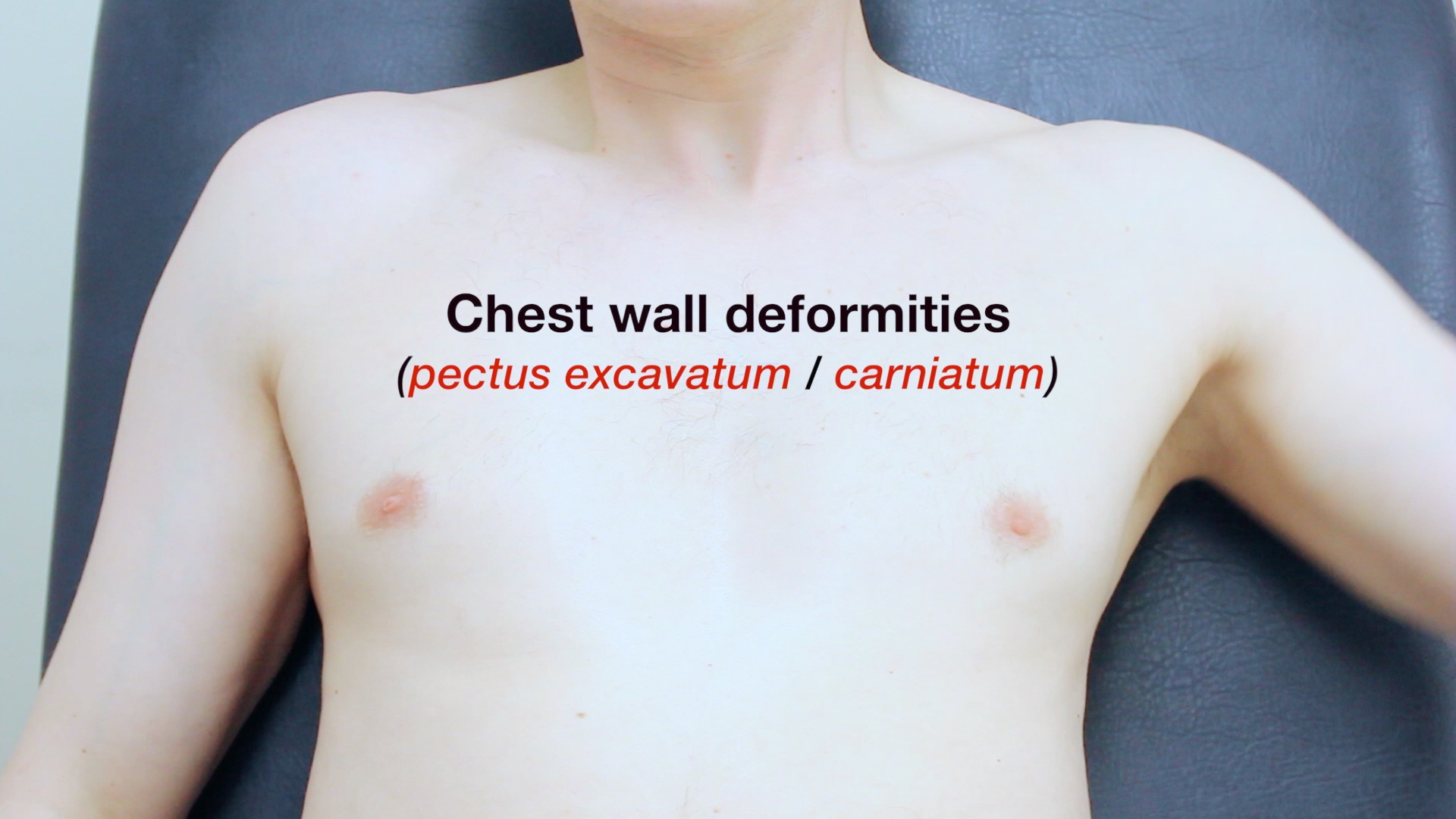
Chest wall deformities – pectus excavatum / pectus carinatum
Visible pulsations – forceful apex beat may be visible – hypertension/ventricular hypertrophy

Inspect chest for scars

Inspect chest for deformities
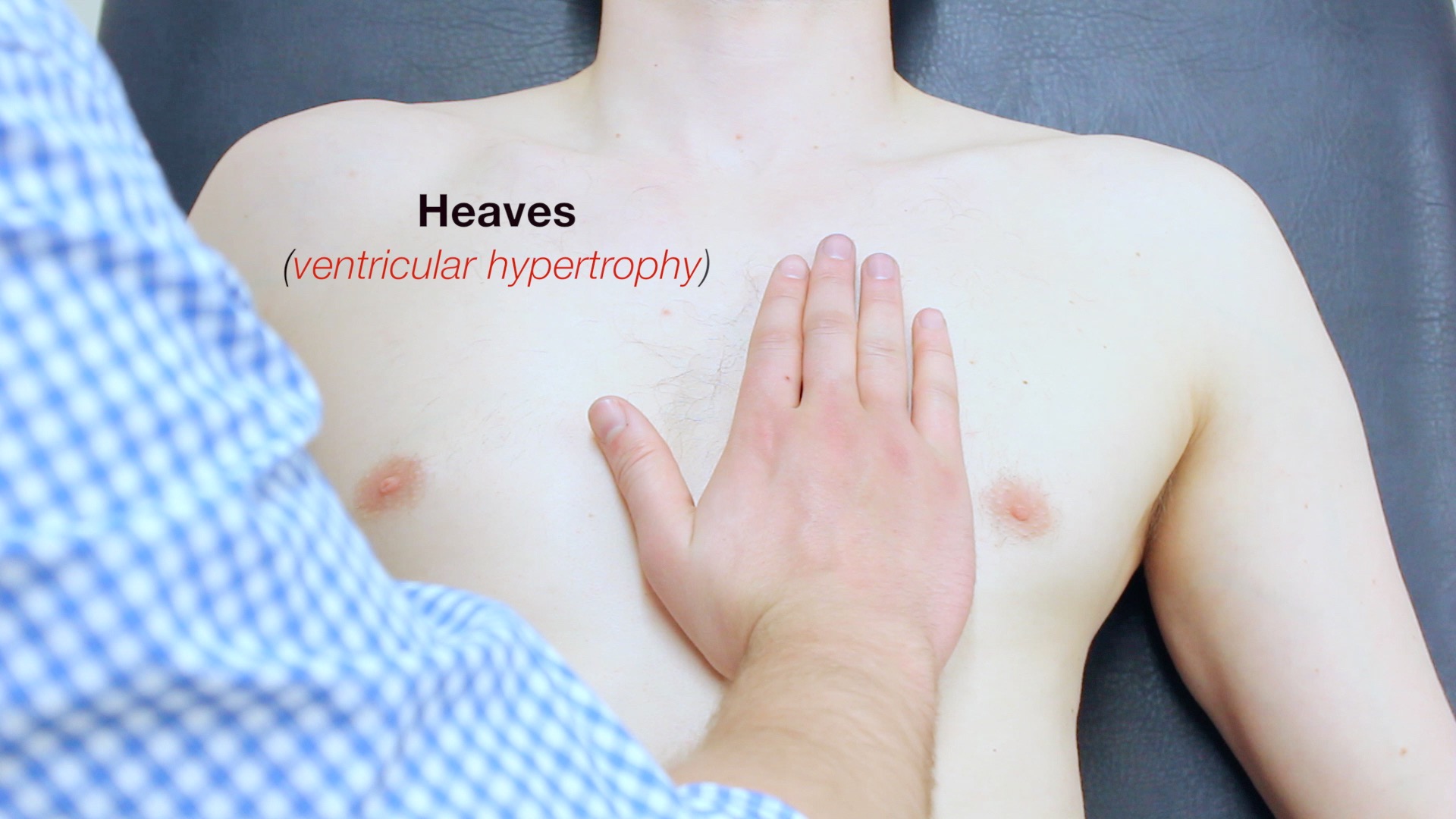
Palpation
Heaves – left sternal edge – ventricular hypertrophy
Thrills – palpable murmurs felt over aortic valve and apex beat
Apex beat:
5th intercostal space / midclavicular line kayak displacement suggests cardiomegaly Once located, count out the intercostal spaces to make it clear to the examiner you have located it

Palpate apex beat

Feel for thrills

Feel for heaves
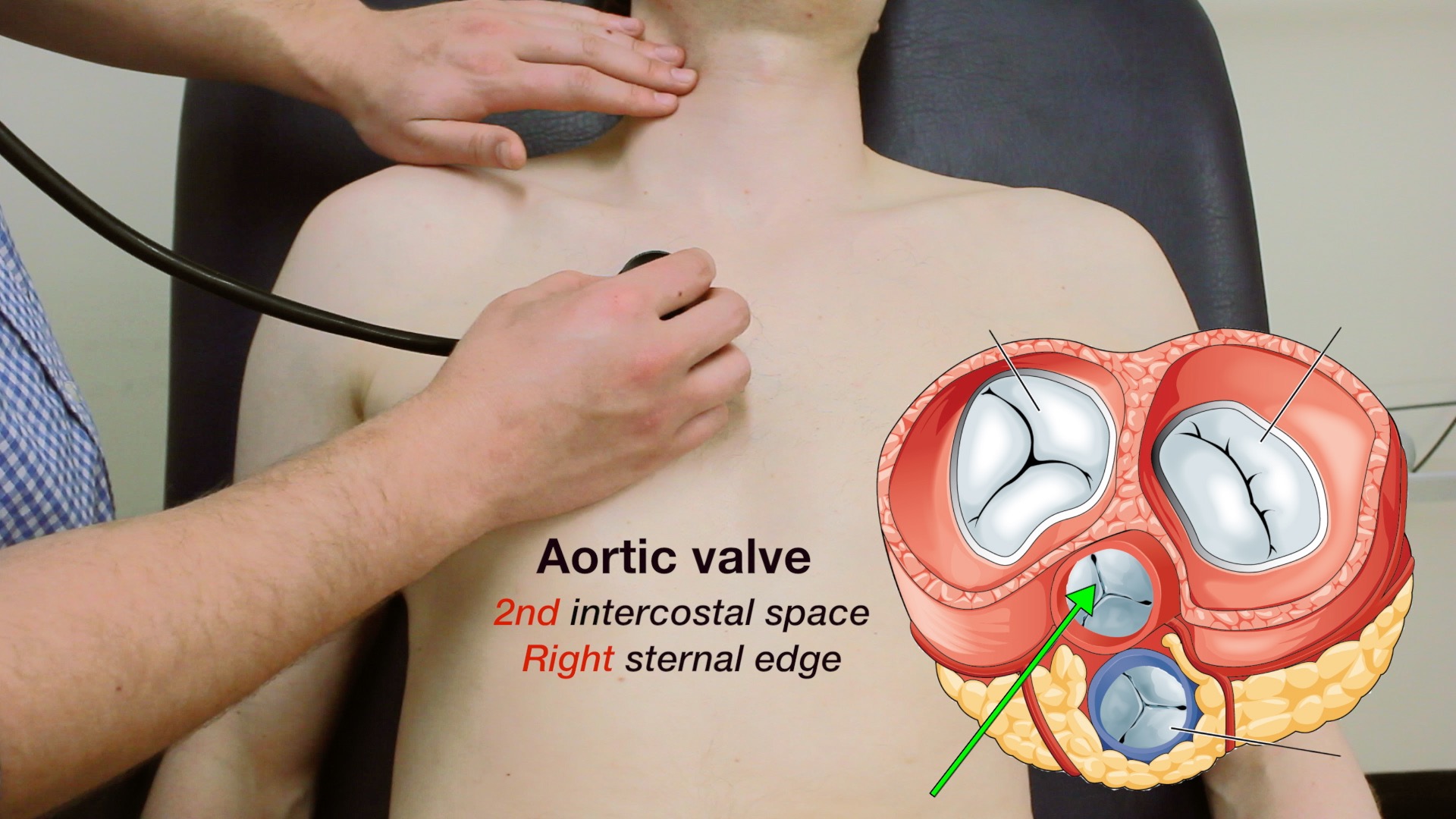
Auscultation
Auscultate the 4 valves
Palpate the carotid pulse to determine the 1st heart sound
Auscultate using the diaphragm of the stethoscope
Auscultate using the diaphragm of the stethoscope
Aortic valve – 2nd intercostal space – right sternal edge
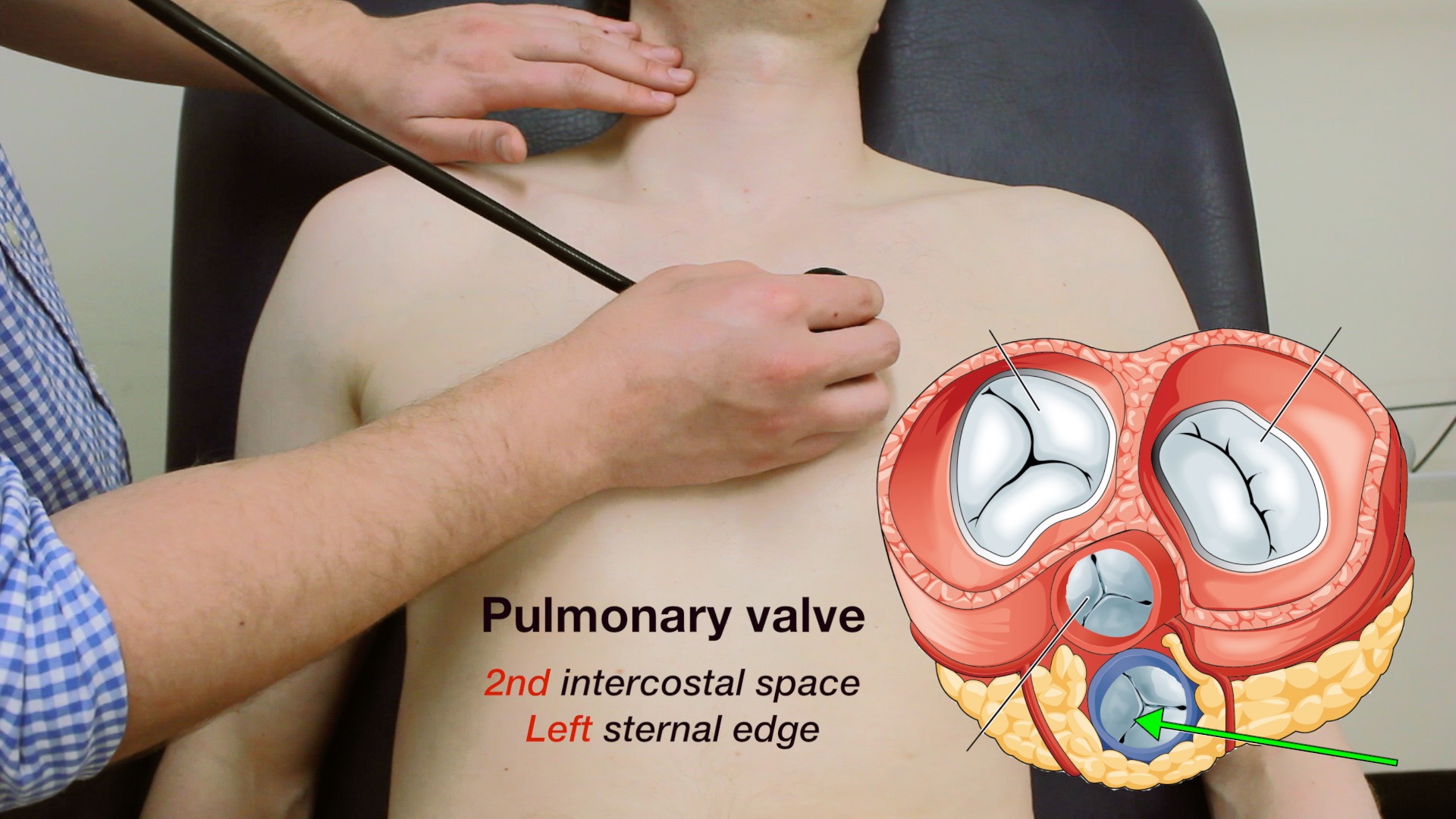
Pulmonary valve – 2nd intercostal space – left sternal edge
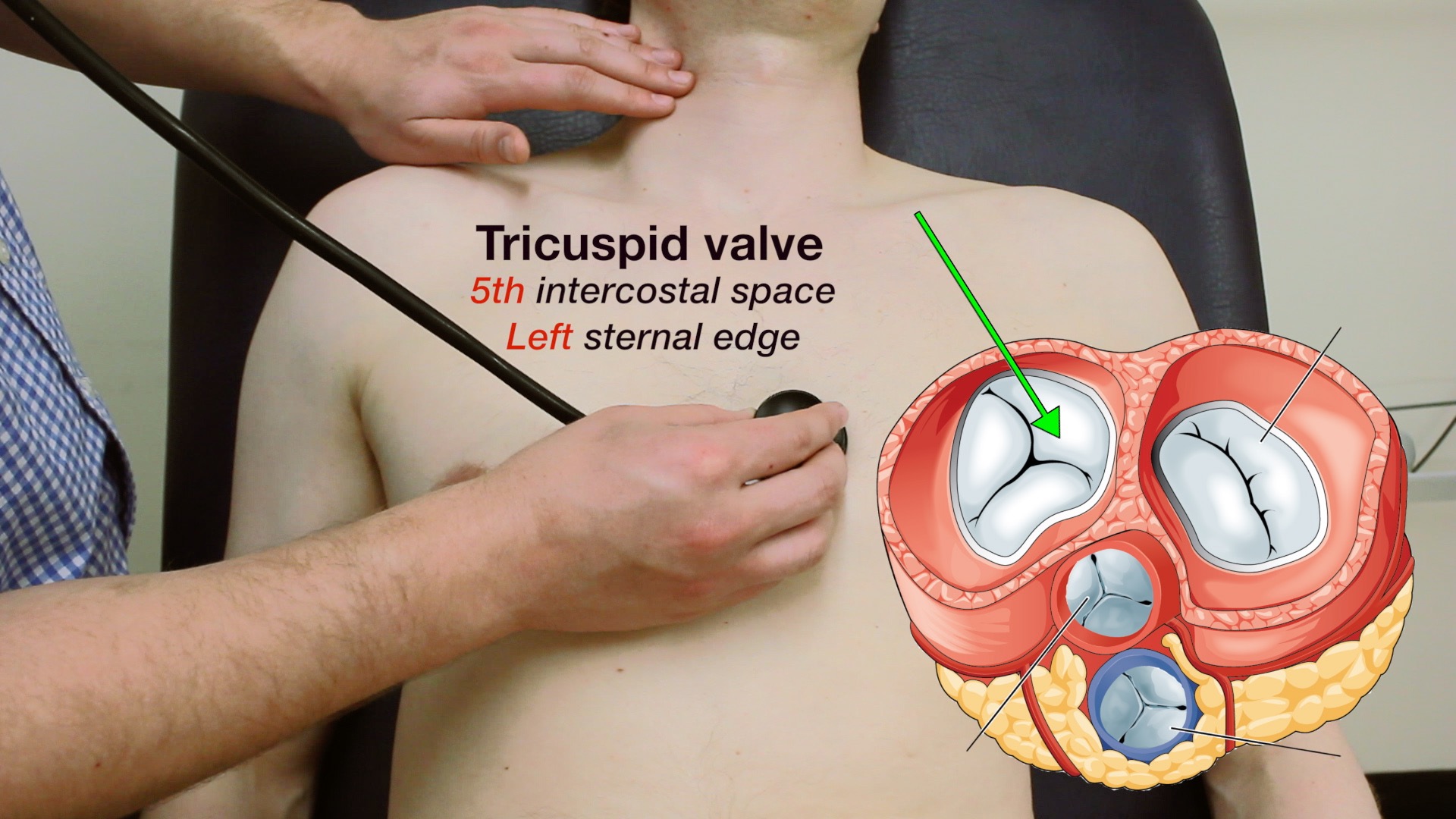
Tricuspid valve – 5th intercostal space – lower left sternal edge
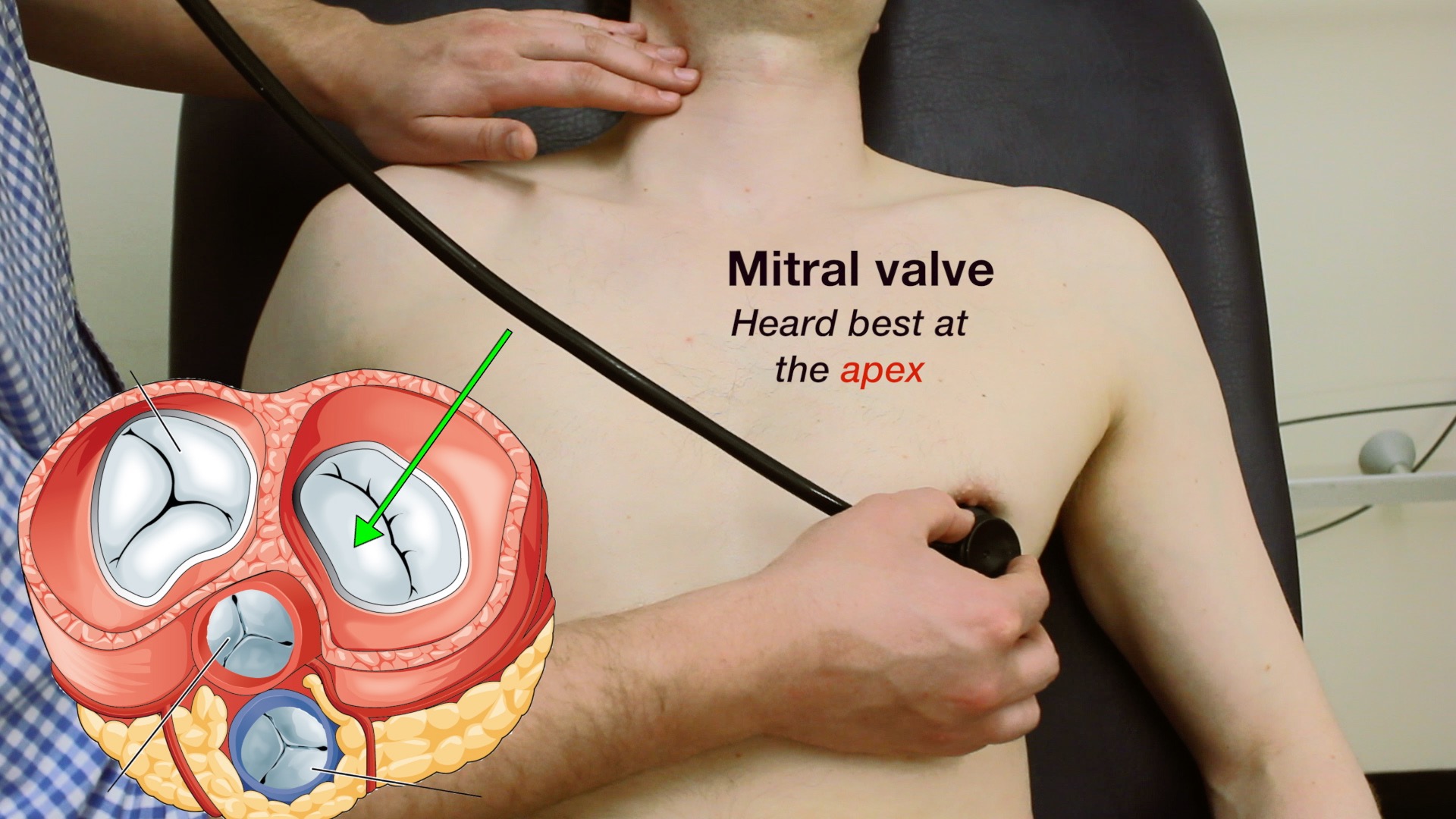
Mitral valve – 5th intercostal space – midclavicular line (apex beat)
Repeat auscultation across the 4 valves with the bell of the stethoscope..

Auscultate aortic valve

Auscultate pulmonary valve

Auscultate tricuspid valve

Auscultate mitral valve

Repeat auscultation with bell
Radiation of the murmur
Carotid arteries (with breath held) – radiation of aortic stenosis murmur
Axilla – radiation of heart murmur into the left axilla – mitral regurgitation
Left sternal edge – aortic regurgitation

Auscultate carotid arteries

Auscultate axilla
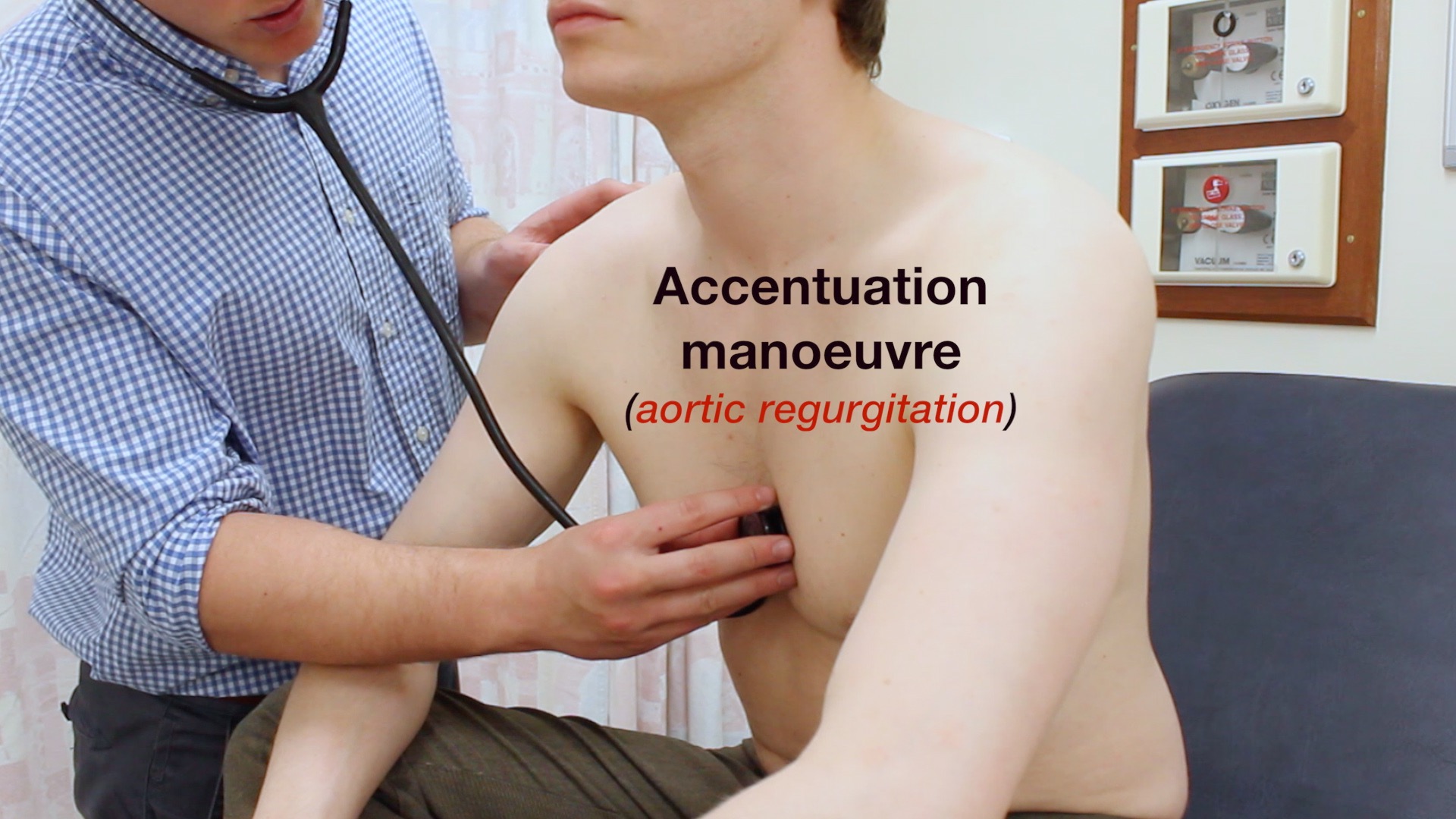
Accentuation maneuvers
These maneuvers cause particular murmurs to become louder DURING expiration
Roll onto left side and listen to mitral area with bell during expiration – mitral murmurs (stenosis and regurgitation)
Lean forward and listen over aortic area during expiration – aortic murmurs are louder (stenosis and regurgitation)
Lean forward and listen over aortic area during expiration – aortic murmurs are louder (stenosis and regurgitation)

Auscultate left sternal edge

Auscultate at heart apex using bell
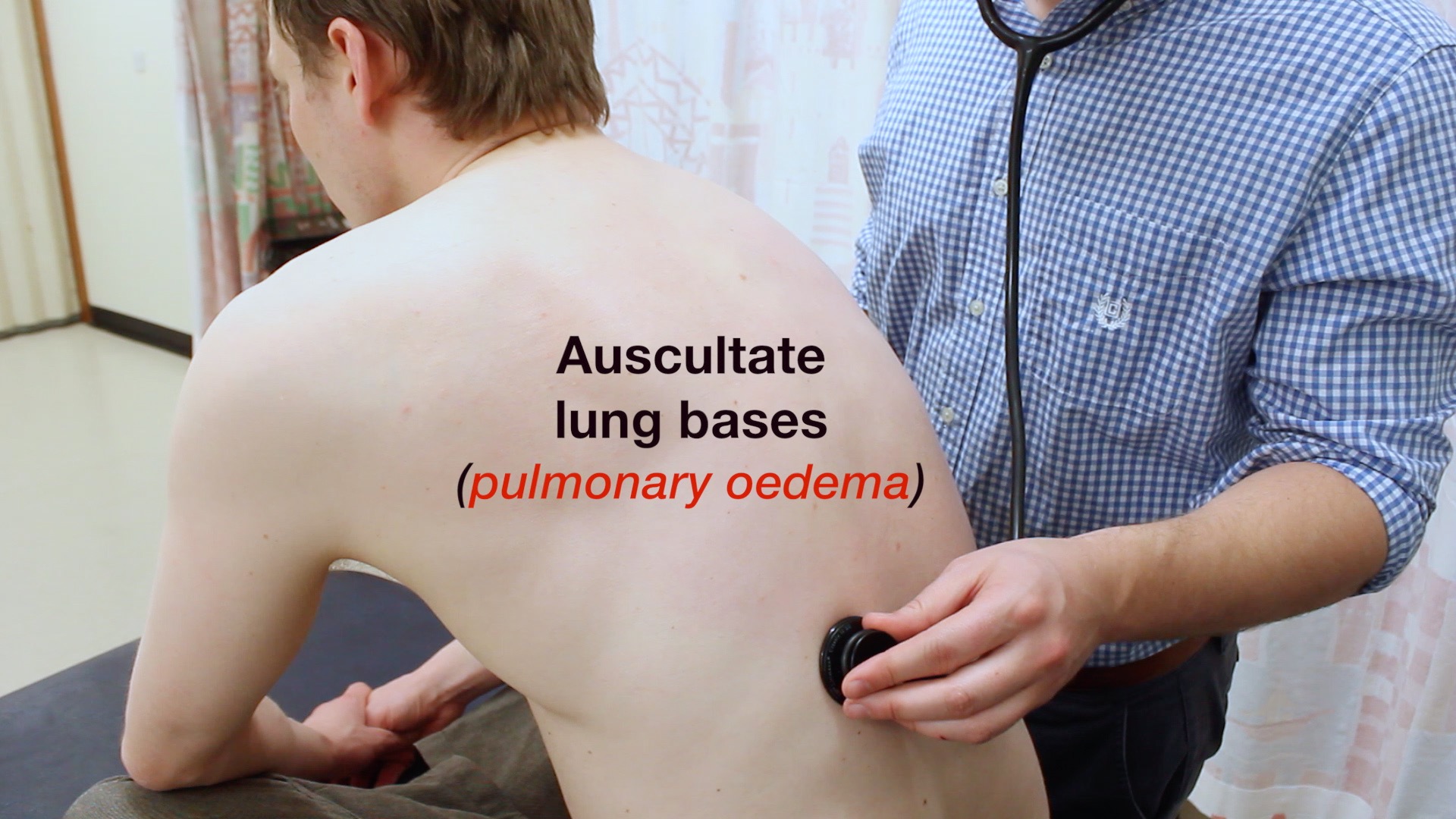
To complete the examination
Auscultate lung bases – crackles may suggest pulmonary oedema – left ventricular failure
Sacral oedema / pedal oedema – may indicate right ventricular failure

Auscultate lung bases

Check for sacral oedema

Check for pedal oedema
Thank patient
Wash hands
Summarise findings
Suggest further assessments and investigations:
Full peripheral vascular examination Record a 12-lead ECG – arrhythmias / myocardial ischaemia
Dipstick urine – proteinuria / haematuria – hypertension
Bedside capillary blood glucose – diabetes
Perform fundoscopy – malignant hypertension – papilloedema
Dipstick urine – proteinuria / haematuria – hypertension
Bedside capillary blood glucose – diabetes
Perform fundoscopy – malignant hypertension – papilloedema
posted by welfare jjambo >> www.welfarejambo.com




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Post a Comment